In contrast to some of the previous topics handled here in the Friday Figure Fix, breasts (or as some might say more casually, boobs, bewbs, boobies, and my personal favorite, "the girls") elicit a stunning variety of feelings and opinions.
For example, if you have a tummy issue, I can pretty much guess that you have a little more tummy than you would like and you want it gone. Whereas with breasts, it could really be anything: too small, too big, too uneven, too droopy, a combination of any of these, or too much like a girl's (for my guy friends out there, you are not forgotten here at this plastic surgery blog!).
So let's tackle one breast-related Figure Fix at a time; we'll start with "
too small".
Now before anyone out there gets too huffy, yes,
breasts are beautiful (we discussed that last time), and yes, size is relative. But let's just imagine that you are a smart, well-adjusted woman who has always felt that she's a bit on the small side for her own figure or a smart, well-adjusted woman who used to be a little bigger (weight loss, pregnancy/nursing, etc) and misses them. You've tried it all: the rolled up sock or wad of tissues in the bra, the "chicken cutlet" gel inserts, the push-up/wonder/water/miracle bras. You've had a friend or two who had "her boobs done" and now you want to know the facts about breast augmentation as they pertain to you.
Lucky you, this blog has the answers to your questions coming right up.
Basics first...
- Can anyone have breast augmentation?
Not exactly. Like I hinted at above, you have to be savvy enough to understand what you're undertaking when you sign the consent form for surgery. You also have to be of age to consent (sorry, all you hopeful 16-year-olds out there, you're just going to have to wait). And, at least for me, you have to be a reasonable person with reasonable expectations.
Of course, if you look around hard enough, you'll find someone who's willing to be a bit more lax in their regard and restrictions. But is that what you really want in your surgeon, someone who prefers the fuzzy side of ethical?
- Is a "boob job" real surgery?
Uh, yeah. By "real surgery", you mean it involves a knife and blood? Yes. There's no magic in making boobs bigger. There will be some pain and soreness afterward. Sorry.
- Who should I see to have this surgery done?
If it were me, I would look for a couple key qualifications: 1) a surgeon, 2) a plastic and reconstructive surgeon.
Generally speaking (and there are always exceptions), plastic surgeons who have completed 5-7 years of specialized surgical training are well qualified to perform breast augmentation (versus other doctors or medical professionals, who may not even be surgeons but claim competence after completing a weekend-type course).
See also answer to question #1, last sentence of second paragraph.
- What exactly are these implants that are going to be stuffed into my chest?
All breast implants approved for use in the United States today are made of the same silicone shell; the major difference that's discussed is what fills those shells. They can be filled with saline (salt water solution, similar to the balance of fluid already in your body) or silicone gel (a squishier non-native substance, whose appearance helped earn the nickname, the "gummy bear"implant).


Photos courtesy of allergan.comOne's saline-filled, the other's silicone-gel filled. Can you tell the difference? Yeah, not so much by looking at a picture - but feeling the implants gives you the obvious answer. The saline-filled one is pretty similar to a water balloon, whereas the silicone-gel filled one is like one of those stress reliever balls you squeeze in your fist. Some say the silicone-gel filled implant mimics the consistency of the human breast more closely.
There are also other, more minor differences in implants. The shape of the implant can be round or what is termed "anatomic".

As you can see in my lovely illustration, the implants when viewed flat on from above look fairly similar in shape (round, or close to round). When the implants are placed on a flat surface and viewed from the side, you can see more of a difference. But when you hold up the implants as if in the position they will assume in an upright woman, the difference between the round and "anatomic" implants are fairly negligible - both resemble the natural breast pretty closely, due to gravity.
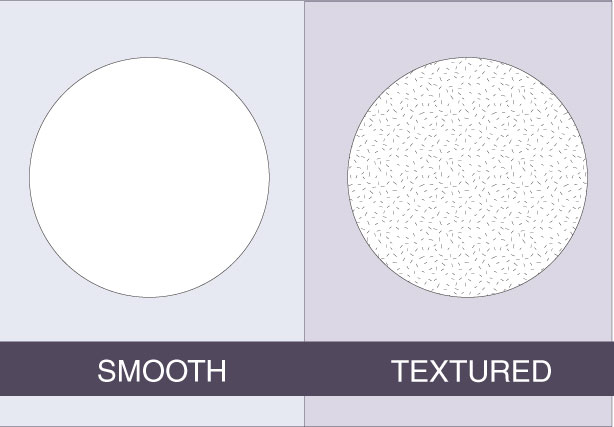
The implant shell can also feel different on the outside, which may or may not affect how the body heals around the implant. Some surgeons will only use smooth-surfaced implants, while others swear by "textured" implants.

The plastic surgical literature doesn't really have much evidence to say that one is "better" than the other, not in hard numbers from clinical trials. So deciding "smooth vs textured" is generally up to the surgeon and you.
- Is this stuff guaranteed?
Well, yes and no. Within a certain time frame, most implant manufacturers will replace implants at no cost if their labs determine that the cause of the implant "failure" is if there was something inherently faulty with the implant itself. Depending on the situation, your surgeon may also waive his/her fee. But that might still leave you responsible for any additional OR and anesthesia fees.
Generally speaking, though, if you wish you had gone bigger (or smaller) after the fact, you might be stuck with paying for the entire surgery all over again.
Other questions? Stay tuned for further Friday Figure Fix installments, or email me at angelinelimmd [at] duetplasticsurgery [dot] com.
 Photo by Juergen Teller for NYMag
Photo by Juergen Teller for NYMag